|
Case Report
Acute exacerbations of myasthenia gravis in COVID-19 infection: A case report on the role of plasmapheresis in preventing intubation
1 Critical Care Division, Anesthesiology and Intensive Therapy Department, Faculty of Medicine, Universitas Indonesia, Cipto Mangunkusumo National General Hospital, Jakarta, Indonesia
2 Anesthesiology and Intensive Therapy Department, Faculty of Medicine, Universitas Indonesia, Cipto Mangunkusumo National General Hospital, Jakarta, Indonesia
Address correspondence to:
Aino Nindya Auerkari
Cipto Mangunkusumo National General Hospital, Jakarta,
Indonesia
Message to Corresponding Author
Article ID: 100134Z06AA2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Auerkari AN, Sugiarto A, Aditianingsih D, Marcelia M. Acute exacerbations of myasthenia gravis in COVID-19 infection: A case report on the role of plasmapheresis in preventing intubation. Case Rep Int 2025;14(2):5–11.ABSTRACT
Introduction: Myasthenia gravis (MG) is an autoimmune condition characterized by the production of autoantibodies against acetylcholine receptors, leading to neuromuscular weakness and potentially life-threatening myasthenic crises. The onset of a myasthenic crisis can result from various triggers, including respiratory infections caused by coronavirus disease 2019.
Case Report: We present a case report detailing the management of a 43-year-old Asian woman with acute exacerbation of myasthenia gravis due to coronavirus disease 2019. The patient was at risk of intubation due to respiratory compromise. Plasmapheresis, a method involving the removal and screening of harmful antibodies, was initiated on the fourth hospital day due to worsening respiratory status despite maximal medical management. Five sessions led to marked improvement and prevented the need for intubation.
Conclusion: Early plasmapheresis can be effective in managing MG exacerbations in severe coronavirus disease 2019 and may prevent intubation when initiated in the appropriate clinical context. This intervention demonstrated notable success in addressing respiratory distress, suggesting its viability as a therapeutic approach in similar scenarios.
Keywords: Case report, COVID-19, Myasthenia gravis, Plasmapheresis
INTRODUCTION
Myasthenia gravis (MG), an autoimmune disorder characterized by muscle weakness due to autoantibodies targeting acetylcholine receptors, poses significant challenges, particularly during acute exacerbations [1]. The emergence of coronavirus disease 2019 (COVID-19) further complicates the clinical management of MG, with respiratory infections acting as potential triggers for myasthenic crises [2]. Plasmapheresis is an effective extracorporeal therapy used to treat myasthenic crises by screening autoantibodies in patients [3]. Plasmapheresis has also been shown to be effective in relieving severe symptoms of COVID-19 infection [4]. In this case report, we present a compelling instance of a patient with severe COVID-19 infection alongside a sudden worsening of MG, resulting in critical respiratory compromise. Urgent intervention is imperative to prevent intubation, leading to the implementation of plasmapheresis as a therapeutic approach.
CASE REPORT
A 43-year-old Asian woman was admitted to the hospital due to worsening shortness of breath over the past week, accompanied by generalized weakness. The patient demonstrated grade 3/5 muscle strength in all four limbs, assessed using the Medical Research Council (MRC) scale, with marked fatigue on repetitive testing. Additionally, the patient reported difficulty opening her eyes especially in the evening, sore throat, and voice changes. She did not have any fever, cough, or gastrointestinal symptoms. The patient had a known history of MG, for which she was taking routine pyridostigmine (60 mg) six times daily and azathioprine (50 mg) twice daily. She also had hypertension and was taking candesartan 10 mg and amlodipine 10 mg daily.
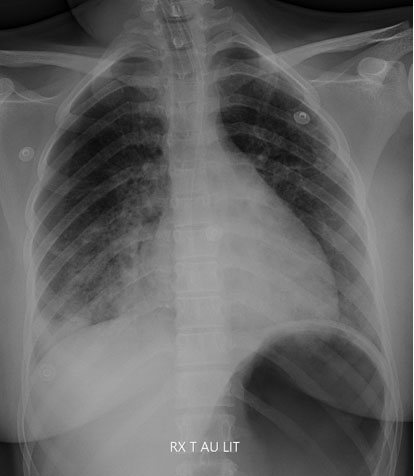
Upon physical examination during admission, the patient was fully conscious and presented with a blood pressure of 130/90 mmHg, a heart rate between 100 and 120 beats/minute, a respiratory rate between 25 and 30 breaths/minute, a temperature of 37 °C, and an oxygen saturation of 98% with the aid of a nasal cannula delivering 3 liters of oxygen/minute. Both eyes showed signs of ptosis. Laboratory examination revealed leukocytosis of 16.010/mm3. The patient tested positive for COVID-19 through a polymerase chain reaction (PCR) test conducted on a nasopharyngeal sample. Chest X-ray examination revealed opacities in both lung fields, as well as a well-defined homogeneous consolidation in the left mid-lower field (Figure 1). The patient was diagnosed with COVID-19 pneumonia with secondary infection and acute exacerbations of MG and was consequently admitted to the ward.
Over a period of three days in the ward, the patient exhibited a deteriorating respiratory condition marked by an increased respiratory rate and oxygen requirements of 15 L/min via a nonrebreathing mask. Consequently, the patient was transferred to the intensive care unit (ICU) for further monitoring and management.
In the ICU, the patient received oxygen therapy through a high-flow nasal cannula at a flow rate of 40 L/min and an oxygen fraction of 80%. The treatments included daily treatment with 100 mg remdesivir for five days, antibiotics for seven days, 15,000 IU heparin for 24 hours, 300 mg amiodarone for 6 hours, 200 mg acetylcysteine thrice daily, and oral supplementation of vitamin D3, vitamin B, and zinc. Plasmapheresis was initiated on the fourth day after clinical worsening despite steroid therapy, with increasing oxygen demand and reduced inspiratory effort observed.
In total, the patient received a total of five sessions of plasmapheresis at two-to-three-day intervals. Plasmapheresis was performed using centrifugation. Following the fifth plasmapheresis session, a subsequent chest X-ray demonstrated a reduction in infiltrates, indicative of therapeutic response (Figure 2). The patient’s ability to perform basic tasks such as lifting arms and speaking in full sentences improved gradually, with documented muscle strength progressing from Grade 3/5 to 4/5 by day 17 of hospitalization. The patient remained hospitalized for a total of 31 days, with 18 of those days spent in the ICU. After being discharged, the patient was doing well and continued to receive outpatient follow-up care. Complete treatment details can be found (Table 1).


DISCUSSION
Myasthenia gravis is an autoimmune disease that results in the development of autoantibodies against acetylcholine receptors at the postsynaptic site. This condition affects 1–20 patients per 100,000 people. The presence of autoantibodies leads to the inhibition of muscle contraction and neuromuscular weakness. The treatment of MG involves the administration of pyridostigmine and azathioprine to control and prevent exacerbations [1].
Myasthenia gravis can be triggered by a variety of factors, with infection being the most common factor, followed by nonadherence to medication and emergency surgery. Respiratory tract infections and gastrointestinal infections are the most frequent infections that can lead to MG exacerbations [3]. Studies have reported an association between coronavirus infection and the exacerbation of autoimmune diseases such as MG, Guillain–Barré syndrome, Bickerstaff’s brainstem encephalitis, and autoimmune meningoencephalitis [4],[5].
Myasthenia gravis exacerbations can range from mild to severe, with the most critical being myasthenic crisis. This condition is characterized by a progressive decline in respiratory function that can be fatal if not treated quickly. In severe cases, adjuvant therapy such as plasmapheresis may be necessary.
Plasmapheresis is an extracorporeal procedure that separates plasma from other blood components to eliminate large molecular weight substrates, including autoantibodies, immune complexes, cryoglobulins, and toxins that accumulate in the plasma. The technique was first used in 1976 for MG therapy, and it has shown promising results in removing autoantibodies directly from the circulation, leading to clinical and functional recovery within a few days [6],[7],[8]. However, plasmapheresis still requires immunotherapy to prevent the overproduction of antibodies in a rebound response. In this case, the patient received methylprednisolone in addition to routine daily azathioprine.
Apart from screening for autoantibodies, plasmapheresis is also useful for filtering inflammatory substrates found in severe viral and bacterial infections. In patients with moderate-to-severe COVID-19 infection, the levels of cytokines such as IL-1, IL-6, IL-2, IL-7, IL-10, G-CSF, MCP 1, MIP-1a, and TNF-a increase, and the levels of inflammatory marker proteins such as C-reactive protein (CRP), aspartate aminotransferase, creatine kinase, creatinine, ferritin, and D-dimer increase. These increased levels of inflammatory substrates are similar to those observed in septic patients. This condition is often associated with respiratory failure and the need for ICU care [9],[10].
Plasmapheresis can be performed by centrifugation or filtration, and the replacement fluid used is generally crystalloids, colloids, albumin, or blood products. For this patient, a centrifugation method was used, and 5% albumin was selected as the replacement fluid due to its ease of use.
Substrates that can be removed from plasma are typically large ones, generally above 40–50 kDa [11]. Autoantibodies in MG have a molecular weight of 20–50 kDa, whereas inflammatory markers such as IL-6 are 21–54.6 kDa, D-dimers are 180–240 kDa, and procalcitonin is 12.8 kDa [12],[13],[14]. Bacterial endotoxins are typically 20–150 kDa [15],[16], while the dimensions of the COVID-19 virus are 60–140 nm, making them large enough to be separated from plasma [17].
Plasmapheresis has been reported to be effective in treating MG, sepsis, and COVID-19. The beneficial effect of this therapy is derived from its physical–mechanical role in influencing autoantibody level immunopathogenesis, filtering cytokine load, and reducing procoagulant agents [3].
A study conducted by Hashemian et al. revealed that in patients with severe COVID-19 who were not intubated, plasmapheresis significantly decreased the levels of inflammatory mediators and acute phase proteins, also improved the PaO2/FiO2 ratio. All the patients in this group recovered. However, in the group of patients who were already intubated, the therapy led to reduced substrate levels but did not result in full recovery, with several patients in that group dying. This indicates that plasmapheresis may be more effective in critically ill COVID-19 patients who have not been intubated [18].
Studies have shown that plasmapheresis can decrease inflammatory markers, reduce oxygen demand, and reduce vasopressor requirements in critically ill COVID-19 patients [19],[20]. In another study in Oman, patients who underwent plasmapheresis were extubated more often and had less mortality [21]. In COVID-19 patients with concomitant exacerbations of autoimmune meningoencephalitis, most patients recover to their initial state after several cycles of plasmapheresis [4].
D-dimer is a product of fibrin degradation that indicates a high risk of thrombosis and is a predictor of mortality in COVID-19 patients [22],[23]. Although the administration of heparin can reduce its production through the inhibition of factor Xa and factor II, it cannot affect the already formed D-dimer. The molecular weight of D-dimer is large enough, so it can be reduced by plasmapheresis [24]. In a study of 3 patients with severe COVID-19 patients with elevated D-dimer levels, plasmapheresis significantly reduced D-dimer levels [25]. By lowering the procoagulant protein, the anticoagulant protein level can be rebalanced. If performed early, disease progression can be prevented, and hemostasis can be improved [26].
Plasmapheresis has also been reported to affect viral load in certain patients. In one study, plasmapheresis via a double filtration method in hepatitis C patients reduced viral ribonucleic acid (RNA) levels. The size of the SARS-CoV-2 virus, approximately 60–140 nm, is also quite large, suggesting that plasmapheresis can help reduce the viral load. However, the primary goal of plasmapheresis in viral infections is to reduce the load to manage the cytokine load and impaired coagulation [17],[18].
To be useful, plasmapheresis initiation should be carried out earlier in the disease phase, as cytokine storms are known to occur more frequently in the first two weeks of illness [27]. Patients who underwent plasmapheresis within the first 12 days of symptom onset had better survival. Therefore, diagnostic testing for cytokine storms should be performed as early as possible, e.g., immediately upon ICU admission, as was done for this patient. Plasmapheresis generally needs to be performed several times, although one cycle of therapy can yield significant results [10],[21].
This case report discusses the use of plasmapheresis in a patient with severe COVID-19 infection and exacerbation of MG. The patient underwent plasmapheresis early on the fourth day after admission. The therapy was administered in 5 sessions with the same dose 2–3 days apart for each session. After the first session, there was a significant improvement in the general weakness and respiratory symptoms, characterized by a decrease in the respiratory rate. The patient was maintained with a high-flow nasal cannula and never required intubation throughout the therapy.
Although this patient tolerated therapy well, plasmapheresis poses limitations including the need for specialized equipment and personnel, high cost, and risk of complications such as bleeding, hypotension, or infections related to central line placement.
Although this patient tolerated therapy well, plasmapheresis poses limitations including the need for specialized equipment and personnel, high cost, and risk of complications. Studies have shown that the side effects of plasmapheresis occur in up to 30% of patients, with most being mild to moderate [28]. Complications may arise from vascular access, replacement fluids, citrate, and plasma product transfusions and may manifest as hypocalcemia, metabolic alkalosis, paresthesia, nausea and vomiting, or muscle disturbances. Hemodynamic instability or allergic reactions to plasma product transfusions may also cause hypotension or vasovagal effects [28],[29]. In this study, the patient was given calcium supplementation to prevent hypocalcemia due to the citrate used in the circuit.
In addition to these hemodynamic and metabolic complications, plasmapheresis carries procedural risks associated with the insertion of an indwelling double-lumen catheter. These include central line-associated bloodstream infections and mechanical complications such as pneumothorax or injury to surrounding tissues during catheter placement. To minimize these risks, strict adherence to aseptic technique and careful procedural planning are essential [29].
Plasmapheresis may significantly reduce circulating levels of certain medications, particularly those with low volumes of distribution and high plasma protein binding. Remdesivir, which is around 88–93% protein-bound, and corticosteroids like methylprednisolone, are susceptible to clearance via plasmapheresis, potentially reducing their efficacy [29]. Hence, careful timing of drug administration relative to the plasmapheresis procedure or dose adjustments may be required to maintain therapeutic levels. While drug levels were not monitored due to facility limitations, this remains a key consideration for future management strategies.
In acute life-threatening exacerbations of MG, intravenous immunoglobulin (IVIG) and thymectomy are other treatment options. Studies have shown that IVIG can be equally as effective as plasmapheresis in such cases, and it can also be used as an adjuvant therapy in the treatment of COVID-19. While both plasmapheresis and IVIG are effective for managing myasthenic crisis, plasmapheresis has been associated with faster clinical improvement in severe cases, particularly those with respiratory failure. It can reduce pathogenic antibody levels more rapidly, making plasmapheresis more suitable when urgent reversal of symptoms is needed. Plasmapheresis offers several additional advantages in this context: each session can mechanically remove approximately 20–30% of circulating autoantibodies, and its peak therapeutic effect may occur up to two weeks after the final session [30]. This delayed benefit is particularly valuable in progressive disease states.
In contrast, IVIG requires large infusion volumes over five consecutive days, which increases the risk of volume overload and allergic reactions, both of which are particularly undesirable in patients with respiratory distress. Moreover, administering IVIG prior to plasmapheresis carries the risk that the infused immunoglobulin could be removed during subsequent plasma exchange, diminishing its efficacy [30]. By initiating treatment with plasmapheresis, we preserved IVIG as a fallback option if needed, without risking its removal. In our case, this sequencing allowed for optimal therapeutic flexibility while minimizing physiological burden.
Importantly, our goal was to prevent intubation. Mechanical ventilation in MG patients poses significant risks, including airway trauma leading to edema, atrophy or dysfunction of respiratory and bulbar muscles prolonging ventilator dependency, and the development of ventilator-associated infections [31]. These potential complications further supported our rationale for using plasmapheresis first in this patient.
Furthermore, in patients with concurrent sepsis or systemic inflammation, plasmapheresis may provide the added benefit of reducing cytokine burden and pro-thrombotic mediators [25]. Nonetheless, IVIG remains a valuable alternative, particularly in settings where plasmapheresis is not feasible. Meanwhile, thymectomy is not recommended for patients with COVID-19 pneumonia and respiratory failure [32].
In this case, plasmapheresis can improve respiratory symptoms, prevent intubation, prevent the progression of sepsis to septic shock, and overall improve patient outcomes. The duration of treatment for this patient was 30 days, with 18 days in the ICU, which is similar to that of the rest of the COVID-19 population undergoing plasmapheresis [21]. The patient was discharged from the ICU on oxygen via a mask and started physiotherapy. On the 31st day of treatment, the patient was discharged for further follow-up as an outpatient.

CONCLUSION
This case underscores the potential efficacy of plasmapheresis in treating severe COVID-19 infection alongside exacerbations of MG. Plasmapheresis exhibited promising outcomes in alleviating respiratory distress, preventing the need for intubation, and enhancing overall patient recovery. The importance of timely intervention, preferably within the initial 12 days of symptom onset, emerges as a critical factor in treatment success. Further investigation is essential to validate these observations and refine therapeutic approaches for similar clinical scenarios.
REFERENCES
1.
Jayam Trouth A, Dabi A, Solieman N, Kurukumbi M, Kalyanam J. Myasthenia gravis: A review. Autoimmune Dis 2012;2012:874680. [CrossRef]
[Pubmed]

2.
Muppidi S, Guptill JT, Jacob S, Li Y, Farrugia ME, Guidon AC, et al. COVID-19-associated risks and effects in myasthenia gravis (CARE-MG). Lancet Neurol 2020;19(12):970–1. [CrossRef]
[Pubmed]
3.
Berrouschot J, Baumann I, Kalischewski P, Sterker M, Schneider D. Therapy of myasthenic crisis. Crit Care Med 1997;25(7):1228–35. [CrossRef]
[Pubmed]
4.
Dogan L, Kaya D, Sarikaya T, Zengin R, Dincer A, Akinci IO, et al. Plasmapheresis treatment in COVID-19-related autoimmune meningoencephalitis: Case series. Brain Behav Immun 2020;87:155–8. [CrossRef]
[Pubmed]
5.
Kim JE, Heo JH, Kim HO, Song SH, Park SS, Park TH, et al. Neurological complications during treatment of Middle East Respiratory Syndrome. J Clin Neurol 2017;13(3):227–33. [CrossRef]
[Pubmed]
6.
Pinching AJ, Peters DK. Remission of myasthenia gravis following plasma-exchange. Lancet 1976;2(8000):1373–6. [CrossRef]
[Pubmed]
7.
Dau PC, Lindstrom JM, Cassel CK, Denys EH, Shev EE, Spitler LE. Plasmapheresis and immunosuppressive drug therapy in myasthenia gravis. N Engl J Med 1977;297(21):1134–40. [CrossRef]
[Pubmed]
8.
Newsom-Davis J, Pinching AJ, Vincent A, Wilson SG. Function of circulating antibody to acetylcholine receptor in myasthenia gravis: Investigation by plasma exchange. Neurology 1978;28(3):266–72. [CrossRef]
[Pubmed]
9.
Harapan H, Itoh N, Yufika A, Winardi W, Keam S, Te H, et al. Coronavirus disease 2019 (COVID-19): A literature review. J Infect Public Health 2020;13(5):667–73. [CrossRef]
[Pubmed]
10.
Balagholi S, Dabbaghi R, Eshghi P, Mousavi SA, Heshmati F, Mohammadi S. Potential of therapeutic plasmapheresis in treatment of COVID-19 patients: Immunopathogenesis and coagulopathy. Transfus Apher Sci 2020;59(6):102993. [CrossRef]
[Pubmed]
11.
Samtleben W, Lysaght MJ. Dialysis techniques: Therapeutic plasma exchange and related techniques. In: Höek WHKK, Lindsay RM, Ronco C, editors. Replacement of renal function by dialysis. London: Kluwer Academic Publishers; 2004. p. 709–24.
12.
Lee PA, Weger GW, Pryor RW, Matson JR. Effects of filter pore size on efficacy of continuous arteriovenous hemofiltration therapy for Staphylococcus aureus-induced septicemia in immature swine. Crit Care Med 1998;26(4):730–7. [CrossRef]
[Pubmed]
13.
Santa Cruz Biotechnology. D-Dimer (DD5): Sc-51864. 2021. [Available at: https://datasheets.scbt.com/sc-51864.pdf]
14.
Maruna P, Nedelníková K, Gürlich R. Physiology and genetics of procalcitonin. Physiol Res 2000;49 Suppl 1:S57–61.
[Pubmed]
15.
Jann B, Reske K, Jann K. Heterogeneity of lipopolysaccharides. Analysis of polysaccharide chain lengths by sodium dodecylsulfate-polyacrylamide gel electrophoresis. Eur J Biochem 1975;60(1):239–46. [CrossRef]
[Pubmed]
16.
Leive L, Morrison DC. Isolation of lipopolysaccharides from bacteria. Methods Enzymol 1972;28:254–62.
17.
Jagdish K, Jacob S, Varughese S, David VG, Mohapatra A, Valson A, et al. Effect of double filtration plasmapheresis on various plasma components and patient safety: A prospective observational cohort study. Indian J Nephrol 2017;27(5):377–83. [CrossRef]
[Pubmed]
18.
Hashemian SM, Shafigh N, Afzal G, Jamaati H, Tabarsi P, Marjani M, et al. Plasmapheresis reduces cytokine and immune cell levels in COVID-19 patients with acute respiratory distress syndrome (ARDS). Pulmonology 2021;27(6):486–492. [CrossRef]
[Pubmed]
19.
Keith P, Day M, Choe C, Perkins L, Moyer L, Hays E, et al. The successful use of therapeutic plasma exchange for severe COVID-19 acute respiratory distress syndrome with multiple organ failure. SAGE Open Med Case Rep 2020;8:2050313X20933473. [CrossRef]
[Pubmed]
20.
Shi H, Zhou C, He P, Huang S, Duan Y, Wang X, et al. Successful treatment with plasma exchange followed by intravenous immunoglobulin in a critically ill patient with COVID-19. Int J Antimicrob Agents 2020;56(2):105974. [CrossRef]
[Pubmed]
21.
Khamis F, Al-Zakwani I, Al Hashmi S, Al Dowaiki S, Al Bahrani M, Pandak N, et al. Therapeutic plasma exchange in adults with severe COVID-19 infection. Int J Infect Dis 2020;99:214–8. [CrossRef]
[Pubmed]
22.
Helms J, Tacquard C, Severac F, Leonard-Lorant I, Ohana M, Delabranche X, et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med 2020;46(6):1089–98. [CrossRef]
[Pubmed]
23.
Zhang L, Yan X, Fan Q, Liu H, Liu X, Liu Z, et al. D-dimer levels on admission to predict in-hospital mortality in patients with Covid-19. J Thromb Haemost 2020;18(6):1324–9. [CrossRef]
[Pubmed]
24.
Diab M, Platzer S, Guenther A, Sponholz C, Scherag A, Lehmann T, et al. Assessing efficacy of CytoSorb haemoadsorber for prevention of organ dysfunction in cardiac surgery patients with infective endocarditis: REMOVE-protocol for randomised controlled trial. BMJ Open 2020;10(3):e031912. [CrossRef]
[Pubmed]
25.
Gucyetmez B, Atalan HK, Sertdemir I, Cakir U, Telci L; COVID-19 Study Group. Therapeutic plasma exchange in patients with COVID-19 pneumonia in intensive care unit: A retrospective study. Crit Care 2020;24(1):492. [CrossRef]
[Pubmed]
26.
Mehta P, McAuley DF, Brown M. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020;395(10229):1033–4. [CrossRef]
[Pubmed]
27.
Yang XH, Sun RH, Zhao MY, Chen EZ, Liu J, Wang HL, et al. Expert recommendations on blood purification treatment protocol for patients with severe COVID-19. Chronic Dis Transl Med 2020;6(2):106–14. [CrossRef]
[Pubmed]
28.
Dogra A, Rana K, Rathod C, Prakash S. Outcome of therapeutic plasma exchange in Myasthenia gravis patients. J Family Med Prim Care 2020;9(12):5971–5. [CrossRef]
[Pubmed]
29.
Mokrzycki MH, Balogun RA. Therapeutic apheresis: A review of complications and recommendations for prevention and management. J Clin Apher 2011;26(5):243–8. [CrossRef]
[Pubmed]
30.
Pavlekovics M, Engh MA, Lugosi K, Szabo L, Hegyi P, Terebessy T, et al. Plasma exchange versus intravenous immunoglobulin in worsening myasthenia gravis: A systematic review and meta-analysis with special attention to faster relapse control. Biomedicines 2023;11(12):3180. [CrossRef]
[Pubmed]
31.
Varelas PN, Chua HC, Natterman J, Barmadia L, Zimmerman P, Yahia A, et al. Ventilatory care in myasthenia gravis crisis: Assessing the baseline adverse event rate. Crit Care Med 2002;30(12):2663–8. [CrossRef]
[Pubmed]
32.
Sanders DB, Wolfe GI, Benatar M, Evoli A, Gilhus NE, Illa I, et al. International consensus guidance for management of myasthenia gravis: Executive summary. Neurology 2016;87(4):419–25. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Aino Nindya Auerkari - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Adhrie Sugiarto - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Dita Aditianingsih - Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Maurin Marcelia - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Aino Nindya Auerkari et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.